
From the 1Department of Rehabilitation Medicine and 2Australian Rehabilitation Research Centre, Royal Melbourne Hospital (RMH), Victoria, and 3Department of Medicine (RMH), University of Melbourne, Melbourne, Australia
Objective: To identify implementation and process issues that influence the implementation of an advance care planning (ACP) programme in rehabilitation settings.
Methods: An ACP programme was established in an inpatient tertiary rehabilitation setting in Victoria, Australia. Rehabilitation patients with chronic illnesses were recruited and the Reach, Effectiveness, Adoption, Implementation and Maintenance (RE-AIM) framework used. Pre-implementation measures included: patient medical record audit of ACP discussions; and barriers and facilitators analyses. Implementation interventions were staff group educational sessions and clinical process changes. Further medical record audit was carried out to review the number of ACP conversations performed and re-evaluate ACP barriers.
Results: A total of 180 consecutive inpatients were recruited for pre- (n = 90) and post- (n = 90) implementation groups. The majority of the pre-implementation cohort were female (51%), mean age 64.2 years (standard deviation 16.4 years) and had low rates of ACP discussions (n = 9, 10%). Major ACP barriers included: lack of staff education programme, and insufficient knowledge to conduct ACP. There was a significant increase in ACP conversations performed (n = 21, 23.3%) between both groups; however, staff reported limited time and skills to perform discussions.
Conclusion: This ACP programme is feasible, but needs robust process evaluation and longer term follow-up to assess the impact of outcomes in public hospital settings on care quality.
Key words: advance care planning; end-of-life care; quality improvement; rehabilitation.
Accepted April 16, 2018; Epub ahead of print Jun 12, 2018
J Rehabil Med 2018; 50: 00–00
Correspondence address: Krystal Song, Department of Rehabilitation Medicine, Royal Melbourne Hospital, Royal Park Campus, 34–54 Poplar Road, Parkville, Victoria, Australia. E-mail: krystal.song@mh.org.au
Advance care planning (ACP) is the process of planning for future healthcare and life-prolonging treatment preferences to guide clinical decision-making when one is unable to communicate decisions due to lack of capacity. We evaluated the effectiveness of an ACP programme in an inpatient rehabilitation setting in Australia with patients with chronic illnesses. This programme identified barriers and enablers, with implementation of ACP strategies in this setting, resulting in an increase in ACP conversations between rehabilitation staff and patients. The programme is feasible, but needs longer-term follow-up to assess the impact of outcomes on improved care quality.
The Australian population aged over 65 years is growing, and is predicted to exceed 20% of the total population by 2033 (1). In Victoria (the second largest state in Australia), approximately 36,000 people die each year and this number will double in the next 25 years. Approximately half of these people will die following chronic life-limiting illnesses, such as heart disease, chronic obstructive pulmonary disease (COPD), cancer, stroke or progressive neurological illnesses (1). Patients with chronic illnesses often experience disabilities, such as fatigue, difficulties with mobility and self-care, and psychological problems (such as depression and anxiety). There are significant implications of these disabilities on functional capacity (and caregivers), with role reversal within families. Chronic illnesses also account for more frequent hospitalizations, longer length of hospital stay, impaired quality of life (QoL) and high financial burden (2).
Advance care planning (ACP) has been identified as an effective tool for future care planning in those with chronic illnesses. It allows patients to communicate their values, beliefs, goals of care, and future treatment preferences in the event that they are unable to do so (3). ACP can take many forms, and in the state of Victoria, Australia, this includes medical enduring power of attorney (MEPOA), statement of choices, refusal of treatment certificate and/or advance directive (AD) (4). ACP enables patient autonomy, shared decision-making processes, and helps ensure that patients receive end-of-life (EOL) care consistent with their life values and goals. ACP also enhances patients’ QoL, encourages better management and coordination of existing resources, improves service provision and ultimately, provides patient-centred care, with reduced stress on families and carers (3–5).
Despite the known benefits of ACP, research has shown it has limited uptake in Australia and internationally (4–6). AD completion rates remain low and range from 5–15% in the general population (7). Patients with chronic illnesses often benefit from palliative care services to improve their QoL; however, these services are limited by poor access, and patients are usually referred late in their illness trajectory. Most patients in later stages of their disease course also lose their cognitive capacity, which limits their ability to participate in EOL decision-making (8, 9). The “neuropalliative rehabilitation” model of care offers a comprehensive and integrated approach to delivery of ACP (10). This model highlights the key supportive role of the rehabilitation multidisciplinary team in discussing ACP with patients, given the expertise of different clinicians in being able to translate wishes and values of patients, aligned with their goals, into a clinical treatment plan.
In rehabilitation settings internationally and in Australia, it is clear that little is known about how ACP processes occur and evidence for the efficacy of ACP interventions (11, 12). To develop, implement and evaluate complex health interventions, such as ACP, requires careful consideration, not only of the outcomes, but also of the processes involved (13). Process evaluation improves understanding of underlying mechanisms related to patients, clinicians, context and intervention delivery, which may have an impact on programme results and sustainability in practice (14). ACP contains multiple interacting components, including heterogeneity of patients, multimodal ACP components, ethical and legal considerations, as well as cultural and religious factors that may lead to a range of possible outcomes. Lack of impact may thus reflect programme implementation failure, rather than ineffectiveness of the programme (15).
The Reach, Effectiveness, Adoption, Implementation and Maintenance (RE-AIM) implementation framework addresses important aspects in process evaluation to help translate research into evidence-based practice, and helps plan programmes to be realistic to adopt in relevant clinical settings (16). Given that most rehabilitation patients have chronic illnesses that require ACP discussions, and rehabilitation settings offer the best opportunities to deliver ACP, this study aimed to use qualitative and quantitative analyses, in the context of the RE-AIM framework (16), to evaluate the feasibility and effectiveness of a structured ACP programme in an inpatient rehabilitation setting in a tertiary hospital in Victoria, Australia.
Patients were recruited from the inpatient rehabilitation unit of the Royal Melbourne Hospital (RMH), a major tertiary hospital in Victoria, Australia from March to October 2017. This quality improvement initiative was approved by the RMH Human Research and Ethics Committee (HREC 2014.033). The 35-bed tertiary rehabilitation unit receives rehabilitation referrals from the acute medical and surgical wards. A total of 90 patients were identified from the inpatient rehabilitation ward, and consecutively recruited for each pre- and post-implementation group. The inclusion criteria were based on state government guidelines (2): (i) patients with confirmed diagnosis of a chronic life-limiting illness (e.g. stroke, neurodegenerative disorder, heart failure, brain tumours), and/or those with multiple co-morbidities; (ii) age 18 years and above; (iii) willing to participate and able to give informed consent; and (iv) medically stable. Exclusion criteria included those with: (i) severe cognitive impairment; and (ii) severe psychiatric illness that required hospitalization in the past year.
For the written survey and staff focus groups, all 42 members of rehabilitation department staff registered in the department were invited to participate by email and by post. Of those who responded, 5 were selected randomly from each discipline (medical, nursing, allied health) in order to obtain representation from each group.
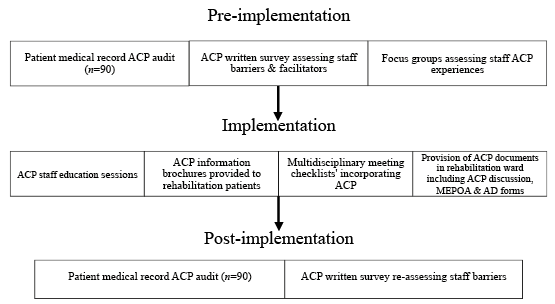
Three phases of implementation were carried out in this ACP programme (Fig. 1). Intervention activities in each phase included:
1) Pre-implementation phase (March – June 2017)
Staff were invited by email to participate in the study. Once they had consented, they were recruited for the focus groups. The primary researcher (KS) conducted ACP discussions involving face-to-face interviews, using open-ended and closed questions to determine staff experience, attitudes and beliefs to ACP implementation. These focus groups were performed in May 2017 in a private meeting room in the rehabilitation ward. These interviews were audiotaped and transcribed by the primary researcher (KS) and information stored in a locked office at the RMH.
2) Implementation phase (July to August 2017)
Each educational session involved the provision of reading materials prior to the session. During the session, the results of the pre-implementation medical record audit were initially presented to allow staff to appraise the current status of ACP discussions with patients and documentation. Furthermore, a didactic teaching session was conducted, using a standardized presentation to demonstrate and describe the key principles of ACP, how to approach and facilitate ACP conversations with patients, documentation forms including AD, and helpful communication skills using ACP videos. In addition, patient and clinician educational resources were provided.
3) Post-implementation phase (September to October 2017)
Fig. 1. Implementation phases. ACP: advance care planning; MEPOA: medical enduring power of attorney; AD: advance directive.
The development, implementation and evaluation of an ACP programme require process evaluation to allow the identification of implementation issues, and contextual factors that may influence outcomes. This allows the adoption of strategies to help translate clinical research findings into routine care. Process evaluation involves the use of both quantitative and qualitative research methods in combination (17, 18), which provide a better understanding of the effectiveness of rehabilitation programmes involving ACP. The use of several indicators that can be linked to programme and service inputs, and programme and service outputs informs a good process evaluation plan. Examples of service inputs include participants (e.g. number, demographic background), setting where services are provided (e.g. inpatient, outpatient), quality of services, and intervention delivery (e.g. type, fidelity to plan). Examples of service outputs include service completion and intervention (e.g. satisfaction) (19). Each of the process indicators maps directly back onto a programme logic model and key process evaluation questions.
Fig. 2 outlines the programme logic for ACP programme, including the programme inputs, activities and potential impacts. The programme logic was developed and reviewed at different times in the programme cycle: before the programme started, during implementation and as part of the programme evaluation.
Fig. 2. Programme logic diagram. ACP: advance care planning; MEPOA: medical enduring power of attorney; AD: advance directive.
1) Reach, Effectiveness, Adoption, Implementation and Maintenance framework
2) Outcome measures
Pre-implementation phase
Information regarding ACP barriers and facilitators, as well as staff experiences with ACP were collected through a combination of qualitative staff survey feedback forms and focus group discussions.
Medical record audit data collected included: patient-related variables (demographic, medical information, level of cognitive impairment, etc.), presence of ACP discussions from progress notes, presence of MEPOA nomination, and AD documentation on electronic medical record system.
ACP barriers and facilitators were explored through staff focus group discussions.
Fig. 3. Five steps of programme evaluation using the Reach, Effectiveness, Adoption, Implementation, Maintenance (RE-AIM) framework (14).
Table I. Process evaluation questions related to Reach, Effectiveness, Adoption, Implementation, Maintenance (RE-AIM) domains and associated data collection tools
Descriptive summary statistics were generated for pre- and post-implementation patient medical record audit results. For the staff ACP survey and focus group discussions, qualitative analysis of rehabilitation staff barriers and facilitators to ACP implementation was performed and described descriptively. Specifically, interview transcripts from focus group discussions in both pre- and post-implementation phases were analysed, coded and interpreted using thematic analyses. Thematic analysis is based on an inductive process that allowed for themes to emerge, and to enable management of large amounts of qualitative data in a credible and robust manner. Transcripts were individually read, “open” coded and emergent thematic features were collectively discussed, categorized and summarized under each topic domain by 2 investigators (KS, FK) until agreement was reached.
A total of 180 patients were enrolled in this study, with 90 patients in each pre- and post-implementation group. The socio-demographic and disease characteristics of both patient cohorts are demonstrated in Table II. Both groups were well-matched for demographic and clinical characteristics, with no drop-outs recorded.
Table II. Pre- and post-implementation audit results (n = 180)
1) Pre-implementation group
The mean age of participants in this group was 64.2 (standard deviation (SD) = 16.4) years, with 51.1% female. The common diagnoses in this group were: orthopaedic (n = 42, 46.7%) and stroke (n = 17, 18.9%). Only 9 patients (10%) had documented ACP conversations. Furthermore, only 7 patients (7.8%) had a MEPOA; and AD was completed in only 3 patients (3%) (Table II).
2) Post-implementation group
Following implementation phase interventions, the post-implementation audit results demonstrated mean age of participants was 66.4 (SD 15.9) years, with 41% being female. Similar to the pre-implementation group, the most common diagnoses on admission were: stroke (n = 25, 27.8%) and orthopaedic (n = 24, 26.7%).
There was an increase in ACP conversations post-implementation, with 23.3% (n = 21) of patients having had documented ACP discussions with rehabilitation staff. There were no significant increases in MEPOA nomination and AD completion rates (Table II). The majority of ACP discussions occurred in males (n = 13, 62%), predominantly in those over the age of 60 years (n = 17, 82%), and in those with stroke (n = 12, 57.1%).
Different interventions used in the 3 implementation phases are demonstrated in Fig.1. The results of the pre- and post-implementation phase ACP barriers and facilitators were analysed qualitatively and findings included:
1) Pre-implementation phase
Healthcare provider characteristics. Twenty-six (n = 26, 61.9%) out of 42 rehabilitation staff participated in the pre-implementation written survey, which assessed barriers and facilitators to ACP implementation. There were 8 (30.7%) medical, 13 (50%) nursing and 5 (19.2%) allied health staff. The majority (30.7%, n = 8) were in the 30–39 years age group; 80.8% (n = 21) were female and 53.8% (n = 14) had > 10 years of experience in clinical practice.
Knowledge and use of ACP. Most rehabilitation staff felt that they were “somewhat familiar” with ACP (n = 14). Seven (n = 7) stated that they had never discussed ACP with their patients, with 10 rarely discussing ACP. Most (n = 19) stated that they had not received formal education or training regarding ACP. Rehabilitation staff most commonly discussed ACP when prompted by patient/family (n = 12) and/or after a change in health status (n = 11).
Barriers to effective ACP discussions. The most prevalent provider-level barriers included the lack of a staff education programme (n = 16), not having the knowledge or skills the discussion (n = 12), insufficient experience in facilitating discussions (n = 12) and difficulty defining the right moment for ACP discussions (n = 11) (Table III). The most prevalent system-level barriers were the lack of ACP awareness campaigns in the organization (n = 12) and limited electronic health record capability to track conversations (n = 8).
Facilitators to effective ACP discussions. The most common facilitators include the increasing understanding of ACP discussions (n = 17) and ability of ACP to improve clinical care for patients (n = 14) (Table III).
Of the 26 people who responded to the ACP survey tool, 5 were randomly selected to represent all craft groups within rehabilitation (medical, nursing, allied health). Qualitative analysis of focus group findings indicated that barriers to ACP also included: rehabilitation staff often feeling that patients who have temporary conditions, or young age as not being applicable for initiation of ACP discussions. Some also felt that the rehabilitation setting may not be seen as an appropriate environment to discuss ACP, given that the aim of rehabilitation involves restoration of function and community reintegration rather than discussing EOL issues. In addition, the rehabilitation specialty is often not seen by other specialties and organizational administration as involved in ACP discussions.
2) Post implementation
Qualitative analysis of focus group findings demonstrated ongoing staff barriers to ACP post-implementation. These included limited time and resources, as well as lack of communication skills to perform ACP discussions with patients. Despite these, they continued to feel positive regarding its importance and are motivated to overcome barriers to ACP implementation. They have found that provision of ACP documents improves accessibility and improved the effectiveness of documentation of ACP discussions.
The RE-AIM framework was used to evaluate the ACP programme. The particular elements considered and used for analysis are summarized in Table IV, and the impact of programme discussed.
Table IV. Evaluation of advance care planning (ACP) programme using Reach, Effectiveness, Adoption, Implementation, Maintenance (RE-AIM) framework
To our knowledge, this is the first process evaluation study of an ACP programme established in a rehabilitation setting to inform on its effectiveness, delivery and quality. Consistent with previous ACP studies, the study findings demonstrate the ongoing low uptake of ACP in rehabilitation settings in Australia, including the occurrence of ACP conversations and its components, especially amongst those with chronic illnesses, such as stroke, neurological conditions, cancer, chronic respiratory and cardiovascular disease (4, 11, 12, 20). To address this evidence-practice gap, we implemented a structured ACP programme in a rehabilitation setting in a tertiary hospital in Australia, and used the RE-AIM implementation framework as a process evaluation tool to identify mitigable barriers and implement strategies with contextual adaptations that can be easily adopted in real-life clinical practice (14). The post-implementation findings of this study highlighted the feasibility and positive outcomes of the programme, with increased ACP conversations between rehabilitation staff and patients.
With the increasing emphasis on the integration of EOL skills amongst healthcare providers in Australia, significant cultural and organizational changes are necessary to deliver safe and high-quality EOL care (21). Continuity care providers, such as rehabilitation staff, are uniquely positioned to provide ACP counselling and resources to their patients, as ACP is a longitudinal task optimally facilitated by the provider who is familiar with their condition (10). Rehabilitation is known to have an important role in the treatment and management of most advanced chronic illnesses, such as amyotrophic lateral sclerosis, multiple sclerosis, spinal cord injury, and end-stage lung and heart disease (10). The multidisciplinary team approach allows staff to contribute information about treatments and interventions based on their area of expertise, break the task down into manageable components, assist with problem-solving complex issues using appropriate communication approaches, and use their areas of competency in setting goals of care (2). Often, the unique and uncertain disease trajectories of chronic illnesses, coupled with the high burden of chronically debilitating symptoms and other comorbidities can affect survival, making EOL discussions important as early on as possible. The rehabilitation team is able to help facilitate discussions involving the use of mechanical ventilation, antibiotics, artificial nutrition, and hydration, with the aim of maintaining and/or improving QoL for patients.
The study findings identified multiple staff and systemic barriers in rehabilitation to discussing ACP including limited awareness of ACP and education programmes, as well as the role of rehabilitation in ACP. Despite this, facilitators indicate that rehabilitation staff do perceive its usefulness and are aware of its benefits. These factors encourage continuing and further professional development opportunities for rehabilitation staff in improving ACP knowledge and communication skills, upskilling in best practice EOL care management, with better access to education and training programmes, ACP leadership support for staff, and provision of ACP guidelines and resources. Other recommended rehabilitation service goals include support of governance and administrative initiatives surrounding ACP, mortality and morbidity audits, and quality improvement processes (21). The accessibility of ACP plans is also important and forms a core component of a long-term systemic approach, including ensuring core documentation for transfer of care, system of alerts and triggers to indicate that a person has an ACP, and ease of its accessibility across health services.
It has been shown that patients with chronic illnesses desire communication about ACP and education about topics such as diagnosis and disease process, prognosis, surrogate decision-making, life-sustaining treatments and AD (22, 23). Given the significant number of patients from different cultural and linguistic backgrounds identified in this study, the findings also highlighted that clinicians need to be open to understanding and learning different attitudes and cultural practices in discussing ACP. Education should include specific training for communicating with patients from culturally and linguistically diverse communities and the consideration of their cultural values, beliefs and practices. The use of accredited interpreters is also important to ensure that appropriate and culturally sensitive information is offered and provided.
This study has several limitations. Though the RE-AIM framework is a comprehensive tool for examining programme delivery and effectiveness, it is possible that some implementation processes may affect more than 1 of the 5 domains. For example, rehabilitation staff expertise, beliefs and attitudes may influence effectiveness, adoption and implementation. Some elements of RE-AIM, such as maintenance, were not addressed to their full extent, as implementation of the intervention was not followed up in the long-term to assess other outcomes. It did, however, generate preliminary data to support a future, large-scale intervention trial that can further tailor the ACP interventions, and assess intervention effects on healthcare received and long-term patient outcomes. This study was also not a randomized controlled trial and, hence, did not have any comparator. Potential for both recall bias and respondents’ tendency to provide socially desirable answers cannot be ruled out. However, this was minimized by making survey responses anonymous. Furthermore, this study was conducted in a single rehabilitation inpatient setting, which may limit its generalizability to other settings. However, the use of a formal evaluation framework and well-defined statements of implementation research questions and presentation of clear results and the nature of the programme activities utilized could be feasibly replicated at other institutions.
This pragmatic quality improvement study established the importance of process evaluation when evaluating complex interventions, such as ACP. The findings provided greater explanatory power for the outcomes of an ACP programme and identified process factors requiring further research. It also demonstrated that an ACP education intervention is a feasible way to improve ACP discussions and documentation, and identified key practice-based improvement strategies. The ACP programme aimed to empower rehabilitation staff to drive system changes and build consensus in this complex area, with support from clinical leads. Further robust and larger studies are needed to evaluate the efficacy of the ACP intervention for longer term patient outcomes, and alignment of treatment with the best interests of patients to inform future policies and practice.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize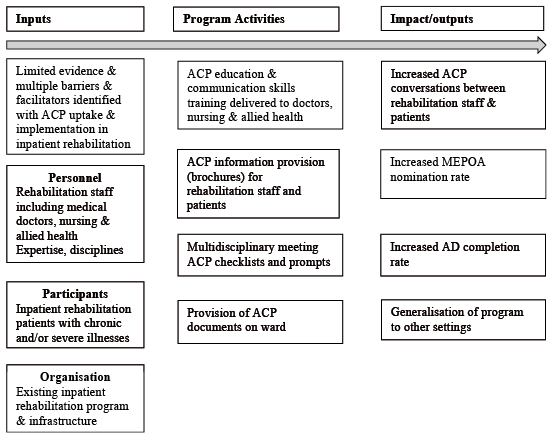 Click to show fullsize
Click to show fullsize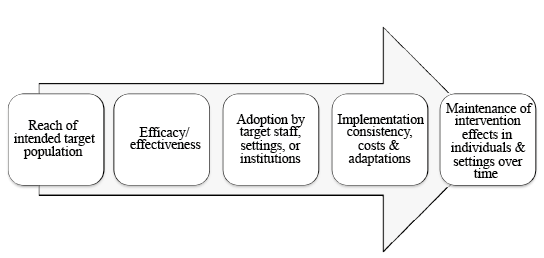 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize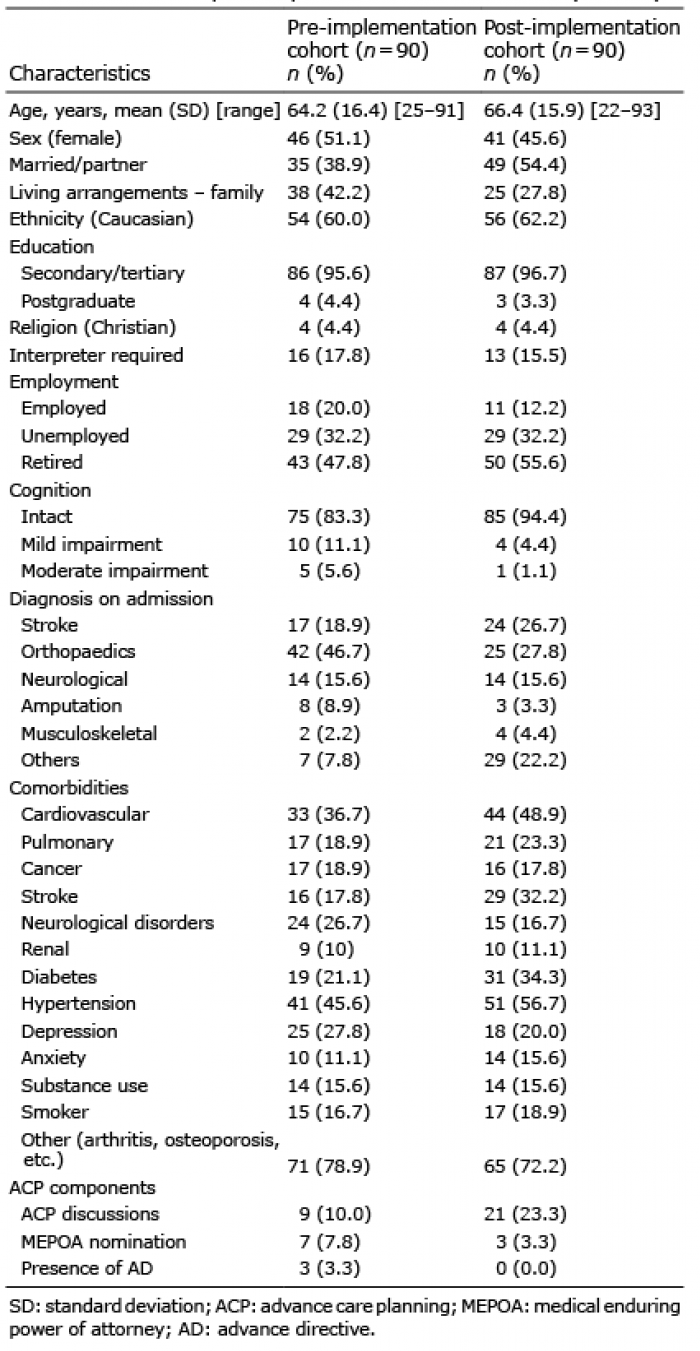 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize